|
| Anovulation |
 |
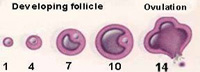
An anovulatory cycle is a cycle during which the ovaries fail to release an oocyte. Therefore, ovulation does not take place. However, a woman who does not ovulate at each menstrual cycle is not necessarily going through menopause. Chronic anovulation is a common cause of infertility.
In addition to the alteration of menstrual periods and infertility, chronic anovulation can cause or exacerbate other long term problems, such as hyperandrogenism or osteopenia. It plays a central role in the multiple imbalances and dysfunctions of polycystic ovary syndrome.
During the first two years after menarche 50% of the menstrual cycles could be anovulatories.
It is in fact possible to restore ovulation using appropriate medication, and ovulation is successfully restored in approximately 90% of cases. The first step is the diagnosis of anovulation. The identification of anovulation is not easy; contrary to what is commonly believed, women undergoing anovulation still have (more or less) regular periods. In general, patients only notice that there is a problem once they have started trying to conceive. |
|
Causes:
Hormonal or chemical imbalance: |
 |
This is the most common cause of anovulation and is thought to account for about 70% of all cases.
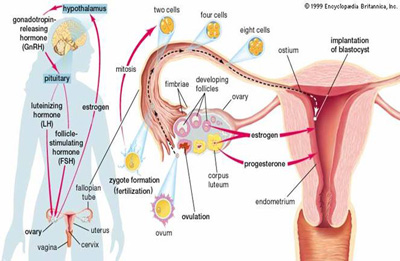
About half the women with hormonal imbalances do not produce enough follicles to insure the development of an ovule. This could be caused by poor hormonal secretions from the pituitary gland or the hypothalamus. |
 |
 |
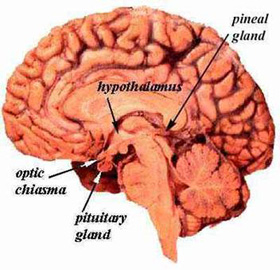
The pituitary gland controls most other hormonal glands in the human body. Therefore, any pituitary malfunctioning affects other glands under its influence, of which the ovaries. This occurs in around 10% of the cases. Mammary glands are also controlled by the pituitary gland, which can thus also affect lactation.
The hypothalamus controls the pituitary gland. In 10% of the cases, alterations in the chemical signals from the hypothalamus can easily seriously affect the ovaries.
There are other hormonal anomalies with no direct link to the ones mentioned above that can affect ovulation. For instance, women with hyper or hypo-thyrodism sometimes have ovulation problems. Thyroid dysfunction can halt ovulation by upsetting the balance of the body’s natural reproductive hormones. Polycystic ovary syndrome (also known as Stein-Leventhal syndrome) and hyperprolactinemia can also cause anovulatory cycles through hormonal imbalances. |
|
Functional problem:
This accounts for around 10-15% of all cases of anovulation. |
| |
The ovaries can stop working in about 5% of cases. This may be because the ovaries do not contain eggs. However, a complete blockage of the ovaries is rarely a cause of infertility. Blocked ovaries can start functioning again without a clear medical explanation. |
| |
A significant emotional shock can temporarily affect the functioning of the brain and can lead to dysfunction of the hypothalamus. However, this is not as common as people might think. |
| |
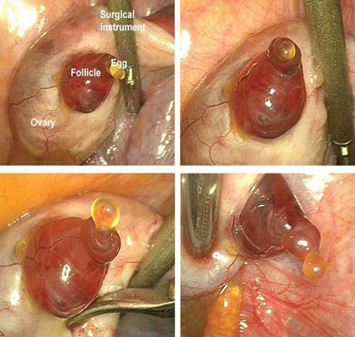
In some cases, the egg may have matured properly, but the follicle may have failed to burst (or the follicle may have burst without releasing the egg). This is called luteinised unruptured follicle syndrome (LUFS). Dr Letouzey from the Arnaud-de-Villeneuve Hospital (CHU) has described the case of a couple with this disorder who goes through IVF, and discusses the different approaches that one might consider for such a diagnosis. |
| |
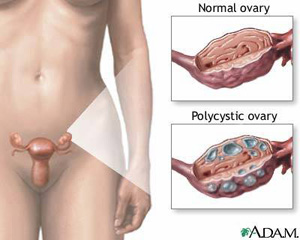
Physical damage to the ovaries, or ovaries with multiple cysts, may affect their ability to function. This is called ovarian dystrophy. Patients who are suffering from Stein-Leventhal syndrome (also referred to as polycystic ovary syndrome, or PCOS) can also suffer from anovulation. Up to 90% of cases of anovulation are caused by PCOS; this syndrome is usually hereditary. |
| |
Weight loss or anorexia can also cause hormonal imbalance, leading to irregular ovulation (dysovulation). It is possible that this mechanism evolved to protect the mother’s health. A pregnancy where the mother is weak could pose a risk to the baby’s and mother’s health. On the other hand, excess weight can also create ovarian dysfunctions. Dr Barbieri of Harvard Medical School has indicated that cases of anovulation are quite frequent in women with a BMI (body mass index) over 27 kg/m2.Unfortunately, not only does excess weight have a negative impact on ovulation itself, but also on treatment efficacy and outcomes of ART (assisted reproductive technique). |
| |
 Detection Detection |
|
Signs and symptoms:
Anovulation is usually associated with specific symptoms. However, it is important to note that they are not necessarily all displayed simultaneously.
Amenorrhea (absence of menstruation) occurs in about 20% of women with ovulatory dysfunction.
Infrequent and light menstruations occur in about 40% of women with ovulatory dysfunction.
Irregular menstruation, where five or more menstrual cycles a year are five or more days shorter or longer than the length of the average cycle.
Absence of mastodynia (breast pain or tenderness) occurs in about 20% of women with ovulatory problems. Increased body and facial hair (this is relatively easy to treat, and is often associated with PCOS, or polycystic ovary syndrome). |
 |
Fertility awareness and LH measurement:
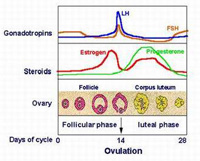
Symptoms-based methods of fertility awareness methods may be used to detect ovulation or to determine that cycles are anovulatory. Charting of the menstrual cycle may be done by hand, or with the aid of various fertility monitors. Records of one of the primary fertility awareness signs—basal body temperature—can detect ovulation by identifying the shift in temperature which takes place after ovulation. It is said to be the most reliable way of confirming whether ovulation has occurred.[13]
Women may also use ovulation predictor kits (OPKs) with detect the increase in luteinizing hormone (LH) levels that usually indicates imminent ovulation. For some women, these devices do not detect the LH surge, or high levels of LH are a poor predictor of ovulation; this is particularly common in women with PCOS. In such cases, OPKs and those fertility monitors which are based on LH may show false results, with an increased number of false positives or false negatives. Dr Freundl from the University of Heidelberg suggests that tests which use LH as a reference often lack sensitivity and specificity. |
|
TREATMENT:
Saravana hospital homoeopathic treatment gives excellent cure for Anovulation. please see the cured reports. |
| back.. |
|
 |
2010 ® Saravana Hospital. All rights reserved . |
|