 |
Asthma |
 |
Asthma is a predisposition to chronic inflammation of the lungs in which the airways (bronchi) are reversibly narrowed. Asthma affects 7% of the population of the United States, 6.5% of British people and a total of 300 million worldwide. During asthma attacks (exacerbations of asthma), the smooth muscle cells in the bronchi constrict, the airways become inflamed and swollen, and breathing becomes difficult. This is often referred to as a tight chest and is a sign to immediately take medication.
Asthma causes 4,000 deaths a year in the United States. Medicines such as inhaled short-acting beta-2 agonists may be used to treat acute attacks. Attacks can also be prevented by avoiding triggering factors such as allergens or rapid temperature changes and through drug treatment such as inhaled corticosteroids and then long-acting beta-2 agonists if necessary. Leukotriene antagonists are less effective than corticosteroids[citation needed], but have no side effects.[citation needed] Monoclonal antibodies, such as mepolizumab and omalizumab, are sometimes effective. Prognosis is good with treatment. |
Although asthma is a chronic obstructive condition, it is not usually considered as a part of chronic obstructive pulmonary disease as this term refers specifically to combinations of bronchiectasis, chronic bronchitis, and emphysema. Unlike these diseases, the airway obstruction in asthma is usually reversible; however, if left untreated, asthma can result in chronic inflammation of the lungs and irreversible obstruction. In contrast to emphysema and bronchiectasis, asthma affects the bronchi, not the alveoli. The National Heart, Lung and Blood Institute defines asthma as a common chronic disorder of the airways characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness (bronchospasm), and an underlying inflammation.
Public attention in the developed world has recently focused on the predisposition because of its rapidly increasing prevalence, affecting up to one quarter of urban children. |
Classification
Asthma is clinically classified according to the frequency of symptoms, FEV1 and peak expiratory flow rate. |
| Clinical classification of asthma severity |
| Severity |
|
Symptom frequency |
|
Nighttime symptoms |
|
Peak expiratory flow rate or FEV1 of predicted |
|
Variability of peak expiratory flow rate or FEV1 |
| Intermittent |
Less than once a week |
Less than twice per month |
More than 80% predicted |
Less than 20% |
| Mild persistent |
More than once per week but less than once per day |
More than twice per month |
More than 80% predicted |
20–30% |
| Moderate persistent |
Daily |
More than once per week |
60–80% predicted |
More than 30% |
| Severe persistent |
Daily |
Frequent |
Less than 60% predicted |
More than 30% |
|
Asthma may also be classified as atopic (extrinsic) or non-atopic (intrinsic), based on whether symptoms are precipitated by allergens (atopic) or not (non-atopic). |
Signs and symptoms |
| Severity of asthma attack |
| Sign/Symptom |
|
Mild |
|
Moderate |
|
Severe |
|
Pending arrest |
| Alertness |
|
May show agitation |
|
Agitated |
|
Agitated |
|
Confused/Drowsy |
| Breathlessness |
|
On walking |
|
On talking |
|
Even at rest |
|
|
| Talks in |
|
Sentences |
|
Phrases |
|
Words |
|
|
| Wheeze |
|
Moderate |
|
Loud |
|
Loud |
|
Absent |
| Accessory muscle |
|
Usually not used |
|
Used |
|
Used |
|
|
| Respiratory rate (/min) |
|
Increased |
|
Increased |
|
Often >30 |
|
|
| Pulse rate (/min) |
|
100 |
|
100-120 |
|
>120 |
|
<60 (Bradycardia) |
| PaO2 |
|
Normal |
|
>60 |
|
<60 ,possible cyanosis |
|
|
| PaCO2 |
|
<45 |
|
<45 |
|
>45 |
|
|
|
Because of the spectrum of severity within the asthma, some people with asthma only rarely experience symptoms, usually in response to triggers, where as other more severe cases may have marked airflow obstruction at all times.
Asthma exists in two states: the steady-state of chronic asthma, and the acute state of an acute asthma exacerbation. The symptoms are different depending on what state the patient is in.
Common symptoms of asthma in a steady-state include: nighttime coughing, shortness of breath with exertion but no dyspnea at rest, a chronic 'throat-clearing' type cough, and complaints of a tight feeling in the chest. Severity often correlates to an increase in symptoms. Symptoms can worsen gradually and rather insidiously, up to the point of an acute exacerbation of asthma. It is a common misconception that all people with asthma wheeze—some never wheeze, and their disease may be confused with another chronic obstructive pulmonary disease such as emphysema or chronic bronchitis.
An acute exacerbation of asthma is commonly referred to as an asthma attack. The cardinal symptoms of an attack are shortness of breath (dyspnea), wheezing, and chest tightness. Although the former is often regarded as the primary symptom of asthma, some patients present primarily with coughing, and in the late stages of an attack, air motion may be so impaired that no wheezing may be heard. When present the cough may sometimes produce clear sputum. The onset may be sudden, with a sense of constriction in the chest, as breathing becomes difficult and wheezing occurs (primarily upon expiration, but sometimes in both respiratory phases). It is important to note inspiratory stridor without expiratory wheeze however, as an upper airway obstruction may manifest with symptoms similar to an acute exacerbation of asthma, with stridor instead of wheezing, and will remain unresponsive to bronchodilators.
Signs of an asthmatic episode include wheezing, prolonged expiration, a rapid heart rate (tachycardia), and rhonchous lung sounds (audible through a stethoscope). During a serious asthma attack, the accessory muscles of respiration (sternocleidomastoid and scalene muscles of the neck) may be used, shown as in-drawing of tissues between the ribs and above the sternum and clavicles, and there may be the presence of a paradoxical pulse (a pulse that is weaker during inhalation and stronger during exhalation), and over-inflation of the chest.
During very severe attacks, an asthma sufferer can turn blue from lack of oxygen and can experience chest pain or even loss of consciousness. Just before loss of consciousness, there is a chance that the patient will feel numbness in the limbs and palms may start to sweat. The person's feet may become cold. Severe asthma attacks which are not responsive to standard treatments, called status asthmaticus, are life-threatening and may lead to respiratory arrest and death.
Though symptoms may be very severe during an acute exacerbation, between attacks a patient may show few or even no signs of the disease. |
Cause
Asthma is caused by environmental and genetic factors, which can influence how severe asthma is and how well it responds to medication. Some environmental and genetic factors have been confirmed by further research, while others have not been. Underlying both environmental and genetic factors is the role of the upper airway in recognizing the perceived dangers and protecting the more vulnerable lungs by shutting down the airway. Profet has argued that allergens look to our immune systems like significant threats. Asthma, in this view, is seen as an evolutionary defense. This view also suggests that removing or reducing airborne pollutants should be successful at reducing the problem.
Environmental
Many environmental risk factors have been associated with asthma development and morbidity in children, but a few stand out as well-replicated or that have a meta-analysis of several studies to support their direct association.
Environmental tobacco smoke, especially maternal cigarette smoking, is associated with high risk of asthma prevalence and asthma morbidity, wheeze, and respiratory infections. Low air quality, from traffic pollution or high ozone levels, has been repeatedly associated with increased asthma morbidity and has a suggested association with asthma development that needs further research. Recent studies show a relationship between exposure to air pollutants (e.g. from traffic) and childhood asthma. This research finds that both the occurrence of the disease and exacerbation of childhood asthma are affected by outdoor air pollutants.
Caesarean sections have been associated with asthma when compared with vaginal birth; a meta-analysis found a 20% increase in asthma prevalence in children delivered by Caesarean section compared to those who were not. It was proposed that this is due to modified bacterial exposure during Caesarean section compared with vaginal birth, which modifies the immune system (as described by the hygiene hypothesis). Psychological stress has long been suspected of being an asthma trigger, but only in recent decades has convincing scientific evidence substantiated this hypothesis. Rather than stress directly causing the asthma symptoms, it is thought that stress modulates the immune system to increase the magnitude of the airway inflammatory response to allergens and irritants.
Viral respiratory infections at an early age, along with siblings and day care exposure, may be protective against asthma, although there have been controversial results, and this protection may depend on genetic context.
Antibiotic use early in life has been linked to development of asthma in several examples; it is thought that antibiotics make one susceptible to development of asthma because they modify gut flora, and thus the immune system (as described by the hygiene hypothesis). The hygiene hypothesis is a hypothesis about the cause of asthma and other allergic disease, and is supported by epidemiologic data for asthma. For example, asthma prevalence has been increasing in developed countries along with increased use of antibiotics, c-sections, and cleaning products. All of these things may negatively affect exposure to beneficial bacteria and other immune system modulators that are important during development, and thus may cause increased risk for asthma and allergy.
Recently scientists connected the rise in prevalence of asthma, to the rise in use of paracetamol, suggesting the possibility that paracetamol can cause asthma.
It has been suggested that viral infections such as HSV, VSV and CSV are correlated to asthma episodes |
|
Many of these genes are related to the immune system or to modulating inflammation. However, even among this list of highly replicated genes associated with asthma, the results have not been consistent among all of the populations that have been tested. This indicates that these genes are not associated with asthma under every condition, and that researchers need to do further investigation to figure out the complex interactions that cause asthma. One theory is that asthma is a collection of several diseases, and that genes might have a role in only subsets of asthma. For example, one group of genetic differences (single nucleotide polymorphisms in 17q21) was associated with asthma that develops in childhood.
Gene–environment interactions
Research suggests that some genetic variants may only cause asthma when they are combined with specific environmental exposures, and otherwise may not be risk factors for asthma.
The genetic trait, CD14 single nucleotide polymorphism (SNP) C-159T and exposure to endotoxin (a bacterial product) are a well-replicated example of a gene-environment interaction that is associated with asthma. Endotoxin exposure varies from person to person and can come from several environmental sources, including environmental tobacco smoke, dogs, and farms. Researchers have found that risk for asthma changes based on a person’s genotype at CD14 C-159T and level of endotoxin exposure. |
| CD14-endotoxin interaction based on CD14 SNP C-159T |
| Endotoxin levels |
CC genotype |
TT genotype |
| High exposure |
Low risk |
High risk |
| Low exposure |
High risk |
Low risk |
low risk bronchitis |
Risk factors
Studying the prevalence of asthma and related diseases such as eczema and hay fever have yielded important clues about some key risk factors. The strongest risk factor for developing asthma is a family history of atopic disease; this increases one's risk of hay fever by up to 5x and the risk of asthma by 3-4x. In children between the ages of 3-14, a positive skin test for allergies and an increase in immunoglobulin E increases the chance of having asthma. In adults, the more allergens one reacts positively to in a skin test, the higher the odds of having asthma.
Because much allergic asthma is associated with sensitivity to indoor allergens and because Western styles of housing favor greater exposure to indoor allergens, much attention has focused on increased exposure to these allergens in infancy and early childhood as a primary cause of the rise in asthma. Primary prevention studies aimed at the aggressive reduction of airborne allergens in a home with infants have shown mixed findings. Strict reduction of dust mite allergens, for example, reduces the risk of allergic sensitization to dust mites, and modestly reduces the risk of developing asthma up until the age of 8 years old. However, studies also showed that the effects of exposure to cat and dog allergens worked in the converse fashion; exposure during the first year of life was found to reduce the risk of allergic sensitization and of developing asthma later in life.
The inconsistency of this data has inspired research into other facets of Western society and their impact upon the prevalence of asthma. One subject that appears to show a strong correlation is the development of asthma and obesity. In the United Kingdom and United States, the rise in asthma prevalence has echoed an almost epidemic rise in the prevalence of obesity. In Taiwan, symptoms of allergies and airway hyper-reactivity increased in correlation with each 20% increase in body-mass index.
Asthma and athletics
See also: Exercise-induced asthma
Asthma appears to be more prevalent in athletes than in the general population. One survey of participants in the 1996 Summer Olympic Games, in Atlanta, Georgia, U.S., showed that 15% had been diagnosed with asthma, and that 10% were on asthma medication.
There appears to be a relatively high incidence of asthma in sports such as cycling, mountain biking, and long-distance running, and a relatively lower incidence in weightlifting and diving. It is unclear how much of these disparities are from the effects of training in the sport. |
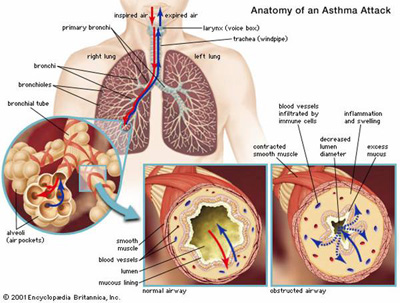
Bronchoconstriction |
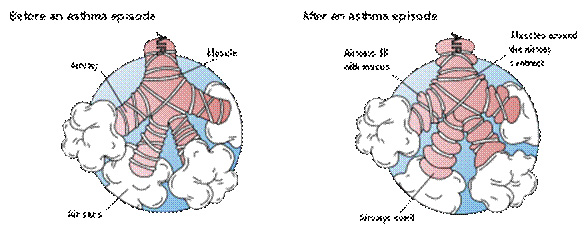 |
Inflamed airways and bronchoconstriction in asthma. Airways narrowed as a result of the inflammatory response cause wheezing.
During an asthma episode, inflamed airways react to environmental triggers such as smoke, dust, or pollen. The airways narrow and produce excess mucus, making it difficult to breathe. In essence, asthma is the result of an immune response in the bronchial airways.
The airways of asthma patients are "hypersensitive" to certain triggers, also known as stimuli (see below). (It is usually classified as type I hypersensitivity.) In response to exposure to these triggers, the bronchi (large airways) contract into spasm (an "asthma attack"). Inflammation soon follows, leading to a further narrowing of the airways and excessive mucus production, which leads to coughing and other breathing difficulties. Bronchospasm may resolve spontaneously in 1–2 hours, or in about 50% of subjects, may become part of a 'late' response, where this initial insult is followed 3–12 hours later with further bronchoconstriction and inflammation.
The normal caliber of the bronchus is maintained by a balanced functioning of these systems, which both operate reflexively. The parasympathetic reflex loop consists of afferent nerve endings which originate under the inner lining of the bronchus. Whenever these afferent nerve endings are stimulated (for example, by dust, cold air or fumes) impulses travel to the brain-stem vagal center, then down the vagal efferent pathway to again reach the bronchial small airways. Acetylcholine is released from the efferent nerve endings. This acetylcholine results in the excessive formation of inositol 1,4,5-trisphosphate (IP3) in bronchial smooth muscle cells which leads to muscle shortening and this initiates bronchoconstriction.
Bronchial inflammation
The mechanisms behind allergic asthma—i.e., asthma resulting from an immune response to inhaled allergens—are the best understood of the causal factors. In both people with asthma and people who are free of the disease, inhaled allergens that find their way to the inner airways are ingested by a type of cell known as antigen-presenting cells, or APCs. APCs then "present" pieces of the allergen to other immune system cells. In most people, these other immune cells (TH0 cells) "check" and usually ignore the allergen molecules. In asthma patients, however, these cells transform into a different type of cell (TH2), for reasons that are not well understood.
The resultant TH2 cells activate an important arm of the immune system, known as the humoral immune system. The humoral immune system produces antibodies against the inhaled allergen. Later, when a patient inhales the same allergen, these antibodies "recognize" it and activate a humoral response. Inflammation results: chemicals are produced that cause the wall of the airway to thicken, cells which produce scarring to proliferate and contribute to further 'airway remodeling', causes mucus producing cells to grow larger and produce more and thicker mucus, and the cell-mediated arm of the immune system is activated. Inflamed airways are more hyper-reactive, and will be more prone to bronchospasm.
The "hygiene hypothesis" postulates that an imbalance in the regulation of these TH cell types in early life leads to a long-term domination of the cells involved in allergic responses over those involved in fighting infection. The suggestion is that for a child being exposed to microbes early in life, taking fewer antibiotics, living in a large family, and growing up in the country stimulate the TH1 response and reduce the odds of developing asthma.
Stimuli
- Allergens from nature, typically inhaled, which include waste from common household pests, the house dust mite and cockroach, as well as grass pollen, mold spores, and pet epithelial cells;
- Indoor air pollution from volatile organic compounds, including perfumes and perfumed products. Examples include soap, dishwashing liquid, laundry detergent, fabric softener, paper tissues, paper towels, toilet paper, shampoo, hairspray, hair gel, cosmetics, facial cream, sun cream, deodorant, cologne, shaving cream, aftershave lotion, air freshener and candles, and products such as oil-based paint.
- Medications, including aspirin,] β-adrenergic antagonists (beta blockers), and penicillin.
- Food allergies such as milk, peanuts, and eggs. However, asthma is rarely the only symptom, and not all people with food or other allergies have asthma Sulfite sensitivity Asthma can occur in reaction to ingestion or inhalation of sulfites, which are added to foods and wine as preservatives.
- Salicylate sensitivity Salicylates can trigger asthma in sensitive individuals. Salicylates occur naturally in many healthy foods. Aspirin is also a salicylate.
- Use of fossil fuel related allergenic air pollution, such as ozone, smog, summer smog, nitrogen dioxide, and sulfur dioxide, which is thought to be one of the major reasons for the high prevalence of asthma in urban areas.
- Various industrial compounds (e.g. toluene diisocyanate ) and other chemicals, notably sulfites; chlorinated swimming pools generate chloramines—monochloramine (NH2Cl), dichloramine (NHCl2) and trichloramine (NCl3)—in the air around them, which are known to induce asthma.
- Early childhood infections, especially viral upper respiratory tract infections. Children who suffer from frequent respiratory infections prior to the age of six are at higher risk of developing asthma, particularly if they have a parent with the condition. However, persons of any age can have asthma triggered by colds and other respiratory infections even though their normal stimuli might be from another category (e.g. pollen) and absent at the time of infection. In many cases, significant asthma may not even occur until the respiratory infection is in its waning stage, and the person is seemingly improving. In children, the most common triggers are viral illnesses such as those that cause the common cold.
- Exercise or intense use of respiratory system—the effects of which differ somewhat from those of the other triggers, since they are brief. They are thought to be primarily in response to the exposure of the airway epithelium to cold, dry air.
- Hormonal changes in adolescent girls and adult women associated with their menstrual cycle can lead to a worsening of asthma. Some women also experience a worsening of their asthma during pregnancy whereas others find no significant changes, and in other women their asthma improves during their pregnancy.
- Psychological stress. There is growing evidence that psychological stress is a trigger. It can modulate the immune system, causing an increased inflammatory response to allergens and pollutants. Cold weather can make it harder for patients to breathe. Whether high altitude helps or worsens asthma is debatable and may vary from person to person.
TREATMENT:
Saravana hospital homoeopathic treatment gives excellent cure for Asthma. |
| back.. |
|
 |
2010 ® Saravana Hospital. All rights reserved . |
|